Extended or Combo Bolus with Loop¶
The majority of meals have most of their blood glucose impact within 2-3 hours after eating. Complex carbohydrates are slowed by their fat and protein content and can lead to extended time of blood glucose impacts. Many people with type 1 are familiar with the late blood glucose spikes from Chinese food, pasta, pizza, or burritos. This extended blood glucose impact can be tricky to properly bolus for in traditional one-bolus insulin delivery.
In traditional multiple daily injection therapy, these complex meals may require additional insulin boluses to help control long, slow absorption meals. The trick is to try to time the second bolus at a time when blood glucose is starting to rise and it can be tricky to estimate how much to give to control the tail end of those slow meals.
If you're using traditional pump therapy, one technique is to use an extended bolus or dual wave bolus for your complex meal's insulin. In this method, a user give a portion of the insulin up front as an initial bolus and the remainder of the insulin is delivered as a pseudo high temp basal for a user-set duration of time. For example, you may give 5 units of bolus up-front and then "extend" 4 units of insulin over the next 60 minutes. In this way, you are providing a more complex bolus to help match the timing of the meal's blood glucose impacts; avoiding early low blood glucose and addressing later high blood glucose.
The transition to Loop use may be confusing at first for these meals since you cannot use an extended/combo bolus and simultaneously have Loop set temporary basals automatically. The good news is that Loop has a bolus calculator that has the ability to emulate an extended bolus situation...and it's implemented with the pizza icon (or any custom carbohydrate absorption that is set longer than 4 hours).
Pizza Icon¶
Example long absorption time bolus¶
For an example of Loop's bolus adjustments using carbohydrate absorption time, let's take a look at an example meal. This is an example of a long absorption complex carbohydrate meal. This is a mushroom (arborio) risotto dish with heavy cream and cheese ingredients. While some white rice can be fairly quick acting, after several times eating this dish, the family has noticed that the meal tends to have a longer duration of impact on blood glucose. Using a "taco" icon (3 hours absorption) was causing slight low blood glucose soon after eating the meal. Therefore, they have been using the pizza icon to enter the meal's carbohydrate absorption time.
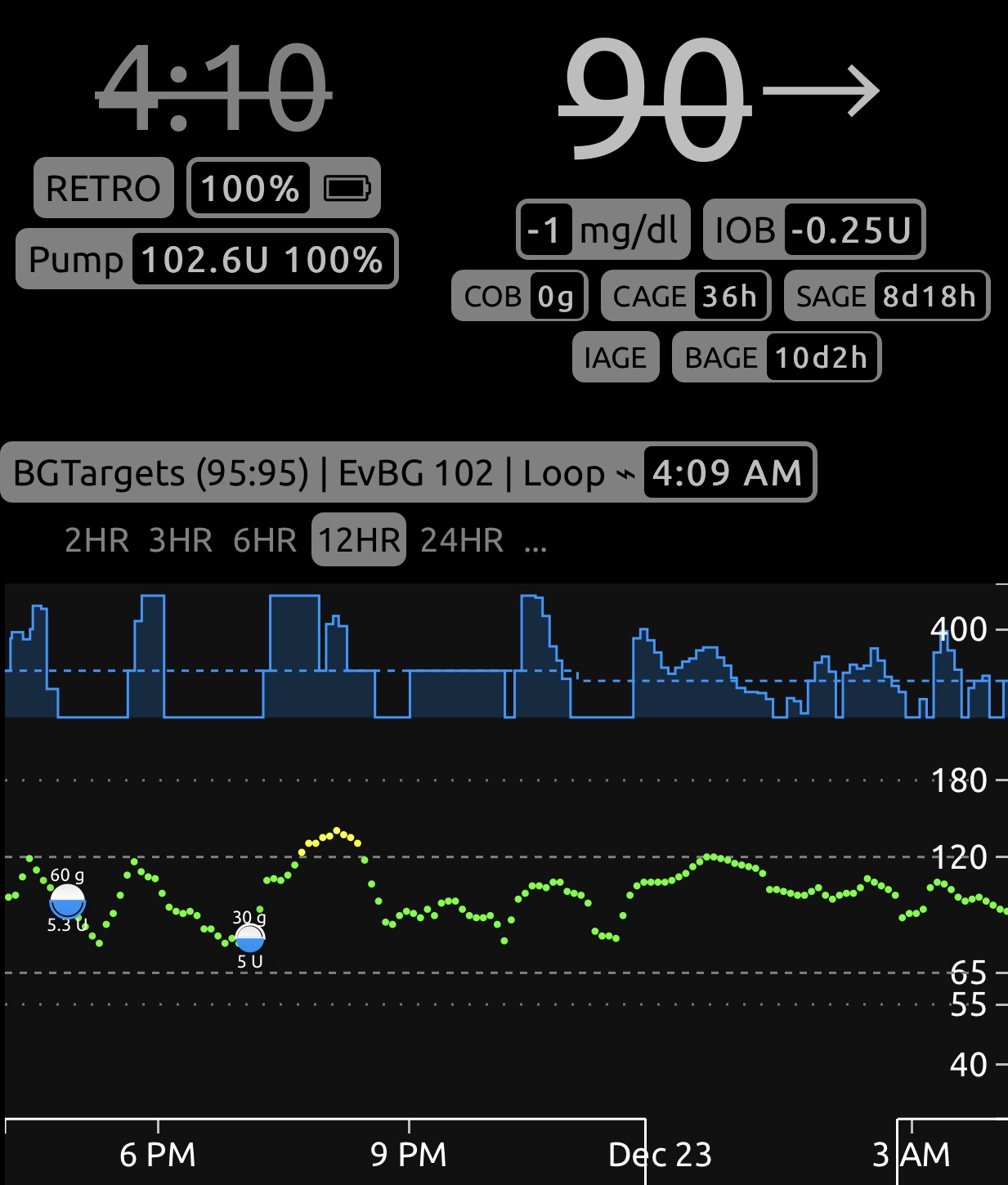
The initial meal entry was 70g at a "pizza" icon absorption time (4 hours). Based on a carbohydrate ratio of 8 g/U, the initial bowl of risotto at 60g should have been a bolus of 7.5 units. Loop recommended 5.3 units or about 70% of the total bolus that would be needed to cover the total carbohydrates. Loop recommended the lower upfront bolus because a full bolus would have overwhelmed the slow absorption of carbohydrates, and the likelihood would be a low blood glucose shortly after eating.
As the meal was being absorbed, Loop was tracking the carbohydrates still remaining to be absorbed and expecting that blood glucose values would be rising soon (knowing that there was still insulin needing to be delivered once safely passed the near-meal low blood glucose potential). Loop would have provided the additional insulin via high temporary basals after seeing blood glucose impacts which indicated the potential for a low blood glucose had passed.
The Loop user then had a second, smaller bowl of risotto about 90 minutes later, and entered 30g at 4 hours absorption again. Notice this bowl of risotto had a bolus recommendation much different than the original bowl. The second bowl had a recommendation of 5 units, much greater amount of bolus relative to the amount of carbs entered than the first bowl had received, and more than the carbohydrate ratio alone would provide (3.75 units). Why the "extra" 1.25 units? Because Loop was including some extra bolus amount to cover what it predicted could safely be provided from the amount not given in the original bowl's bolus (the original bolus was approximately 2.2 units short of the carbohydrate ratio alone recommendation). If the user had not had the second bowl, Loop would have been providing high temporary basals as soon as blood glucose had exceeded the correction range. And in fact, you can see that Loop still provided the remaining insulin via high temporary basals as blood glucose rose after the second bowl, in effect making up the small remaining difference.
Low carb/High Fat or Keto diets¶
The example meal above, while relatively high carbohydrate, also helps illustrate how Loop can be used to bolus effectively for low carb/high fat (LC/HF) or Keto diets. Those diets tend to have low glycemic index food with a relatively long blood glucose impact. Said another way, they don't spike blood sugar as much but often need additional insulin after the meal was eaten to account for the slow conversion of protein to glucose.
To account for those dietary differences, there are two useful strategies:
- convert some of the protein and fat to "equivalent carbohydrates" and
- extend the duration of those carbohydrates using a pizza icon or even longer, depending on the person/food.
Most LC/HF or Keto users will convert a portion of their fat and protein content into an equivalent carbohydrate content. So while an example meal might only have 5g of carbohydrates based on nutritional labels, they may convert 25% of the 20g fat and 50% of the 20g protein grams into an additional 15g of "equivalent carbs" for bolusing purposes. The percentages that people use to convert fat and protein will usually be a bit of trial-and-error, but there are some published articles (here, here, here, and here) that may be helpful starting points if you are interested.